Introduction
Globally, the prevalence of hypertension among adults is 40%, with the highest prevalence (46%) in Africa, and the lowest prevalence (35%) in America. Hypertension is estimated to cause 7.5 million deaths, around 12.8% of the total annual deaths. It is a major risk factor for coronary heart disease, ischaemic and hemorrhagic stroke.1
Global health statistics report 2013 says that in India, 23.1% men and 22.6% women over 25 years suffer from hypertension. Regional studies in India, documents that the prevalence of hypertension ranges from 20-40% among urban adults and 12-17% among rural adults and the number of hypertensives is projected to increase from 118 million in 2000 to 214 million in 2025. In South India, the prevalence of hypertension was reported to be 27.6% among adults in Pondicherry. 2
Because of changes in lifestyle, changes in the environment, the problem of hypertension is increasing. For health care system to plan effective control measures, accurate estimates of hypertension in the community are therefore necessary. Hence, field-based studies become imperative to detect hypertension and its associated factors in order to highlight this problem so that it can be applied for primary and secondary prevention. 3
This study was taken in this direction to estimate the prevalence and associated factors of hypertension among adults aged ≥35 years, so that preventive measure can be initiated to control hypertension and care of high risk general population can be given at community level in the urban service area of multispecialty hospital, Pondicherry Institute of Medical Sciences (PIMS), Puducherry, India. 4, 5, 6, 7
Objective
To assess the pre test knowledge score regarding prevalence of -hypertension among males.
To assess the post test knowledge score regarding prevalence of -hypertension among males
To evaluate the effectiveness of teaching programme on prevalence of -hypertension among males.
To associate between the level of knowledge on prevalence of -hypertension among males with selected demographic variables.
Hypothesis
RH1 – There will be significant difference between pre-test and post-test knowledge score regarding prevalence of -hypertension among males at the level of P≤0.05
RH2 – There will be a significant association of pre-test knowledge score regarding prevalence of -hypertension among males with selected socio-demographical variables at the level of P≤0.05.
Materials and Methods
A sample size of 233 was arrived using the formula n= 4pq/d2, assuming the anticipated prevalence of hypertension to be 30% (based on a study done by Bharati et al.) 8 among ≥35 years aged men and women and a relative precision of 20%.8 The study area was randomly selected ensuring the availability of adequate number of participants required to meet the sample size and achieved a sample size of 236 adults aged ≥35 years.
A house to house survey was done to identify the study participants and were interviewed to collect the information on demographics, personal history and family history was collected using a predesigned, pretested structured questionnaire.
Demographic information included age, sex, marital status, educational status, occupation, nature of occupation, family income, religion, type of family and dietary pattern. Personal history included personal medical history (considered if diagnosis made by Physician) including treatment, perceived stress due to financial problems, family problems, work pressure and among males smoking, tobacco use, and alcohol intake. Family history of hypertension was considered in family history. Socio-economic status was assessed using Kuppuswamy’s Socioeconomic Status Scale.
Physical examination included measurement of blood pressure, anthropometric measurements like height, weight and waist circumference using standard procedures. Blood pressure was measured using electronic blood pressure monitor. The participants were allowed to rest (relax) for 10-15 minutes with legs uncrossed. The blood pressure was measured on the left upper arm and was positioned in such a way that the left upper arm was at the same level with the heart. Two readings were taken in sitting position with 5 minutes rest between each reading and the average of the two was considered. 9, 10, 11, 12
BMI was categorized according to WHO classification, <18.5kg/m2 as underweight, 18.5 - 24.9 kg/m2 as normal weight, 25-29.9 kg/m2 as overweight, 30-34.9 kg/m2 as obesity class I, 35-39.9 kg/m2 as obesity class II, and ≥40 kg/m2 as obesity class III. The abdominal obesity was assessed using "The National, Heart, Lung and Blood Institute" criteria, if waist circumference was >102 cms for males and > 88cms for females.
Hypertension was classified according to JNC VII criteria (Seventh Report of the Joint National Committee), systolic/diastolic blood pressure as hypotension for <90/60 mmHg, normal for 90-119/60-79 mmHg, prehypertension for 120-139/ 80-89 mmHg, Stage I hypertension for 140-159/ 90-99 mmHg and Stage II hypertension for ≥160/100 mmHg. Among individuals on antihypertensive treatment, hypertension status was considered to be controlled if blood pressure was <140/90 mmHg and uncontrolled when ≥140/90 mmHg.12
On an average, 8-10 participants were interviewed per day and the time taken for data collection was approximately 40-50 minutes per study participant. All men and women aged ≥35 years willing to participate in the study were included. Mentally challenged and pregnant women were excluded from the study. All the measurements were taken by the principal investigator itself to reduce inter-observer variability.
The data was analyzed using SPSS Statistical Software (version 2.0). The continuous variables were expressed as Mean + SD and dichotomous/categorical variables were presented as percentages. The estimates were presented with precision estimates. The test of significance used was Chi-square test, a non-parametric test to test for association between hypertension and socio-demographic, anthropometric and clinical variables. Demographic Variables age, gender, marital status, educational qualification, occupation, socio – economic status, religion, type of family, dietary habit, type of occupation with regard to physical activity, family history of hypertension, body mass index, abdominal obesity, history of smoking, history of alcohol, total number of sample 236.
The permission to conduct the study was obtained from Institutional Review Board, College of Nursing, PIMS. A written informed consent was obtained from all the study participants before data collection.
Results
The total number of study participants was 236 and their mean age was 53.7 ± 12.4 years. Around two-third (66.5%) were females. Majority (81.8%) of them were married. Only 18.6% were graduates & above. More than half of them (57.2%) were housewives and only 18.2% were having regular income. Around 47.9% were in high socio economic status (SES) and only 16.9% were in low SES. Majority (90.3%) of them were non-vegetarians.
Nearly one-third of the participants (29.2%) were found to have diabetes mellitus and only 3% had history of other non-communicable diseases like ischemic heart disease, renal diseases, etc. Two-third (63.1%) of the study population reported of perceived stress due to financial problems, family problems, work pressure, etc. The proportion of current smokers and alcoholics among males were 19%, 29.1%, respectively. The family history of hypertension was reported among 46.6% of the participants.
The distribution of study population according to Body mass index (BMI) was 2.1%, 27.6%, 47%, 23.3%, for underweight, normal, overweight, obesity (Class I, II, & III), respectively. The abdominal obesity based on waist circumference was observed in 61.9% (males: 15.2%, females: 49.7%) of the study participants.
Prevalence of hypertension
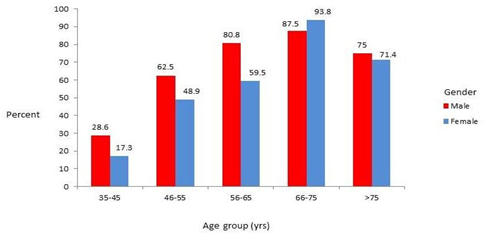
The overall prevalence of hypertension was found to be 52.1% (95% CI: 45.7% - 58.5%) in urban Puducherry, out of which 24% (n=32) were new cases. The mean SBP and DBP were 129.2 mmHg (SD: 16.4) and 78.9 mmHg (SD: 10.4), respectively. Hypertension was reported by 38.6% (old hypertensives) of the study population. The age specific prevalence of hypertension is shown graphically (Figure 1).
Among the known hypertensives, 87.7% reported of taking antihypertensive medications regularly. However, only two-third (58.2%) of those on treatment had blood pressure of <140/90 mmHg (controlled hypertension).
The prevalence of hypertension was 63.3% among males and 46.5% among females. With regard to SES, the prevalence of hypertension was 50% in low SES, 45.8% in middle SES, and 57.5% in high SES.
Hypertension was significantly associated with age, gender, physical activity level with regard to type of occupation, alcohol intake among males, positive family history of hypertension, and abdominal obesity among females.
Statistically significant association was observed between hypertension and sedentary workers, family history of hypertension, abdominal obesity among females, past/current users of alcohol (77.4%) than never users (22.6%).
Discussion
This community based cross sectional study had added strong evidence to the magnitude of hypertension in the union territory of Puducherry, South India. The overall prevalence of hypertension was found to be high (52.1%) in urban population aged ≥35 years in Puducherry. Our study findings was consistent with other Indian studies done by Manimunda et al,13 Vimala et al,14 and Zachariah et al who had observed the prevalence of hypertension to be 50.1%, 47%, and 54.5% respectively. There has been a gradual increase in prevalence of hypertension with time in India and it has been significantly higher among urban adults than their rural counterparts (Figure 2).
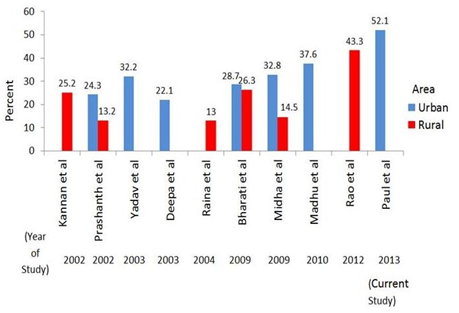
The probable reasons for increasing prevalence are lifestyle changes, environmental factors, rapid urbanization, demographic transition and addictions like tobacco use/ alcohol.
Among the known hypertensives (38.6%), our survey observed that 87.7% were on regular antihypertensive medications but only 58.2% of the old hypertensives had blood pressure under control and 41.8% had uncontrolled blood pressure (SBP ≥140 mmHg and/or DBP ≥90 mmHg). The significantly higher proportion (29.7%) of high blood pressure (undiagnosed hypertension and uncontrolled hypertension) among the general population in the urban community suggests the need for regular community based screening programmes for early detection of hypertension and health education programmes for lifestyle modification to decrease the risk of hypertension in the community.
The prevalence of hypertension was observed to be 20.5%, 52.5%, 68.3%, 91.7%, and 73.3% among those aged 35-45 years, 46-55 years, 56-65 years, 66-75 years, and >75 years, respectively, thus showing a significant increasing trend in prevalence with age (χ2 for trend, p value <0.01). This increasing trend with age is consistent with the other study findings and adds validity to the study.15, 16, 17, 18, 19, 20
With regard to gender, the prevalence of hypertension was significantly higher among males (63.3%) than females (46.5%). And it had been observed in previous studies carried out in India. However, there are few studies where the authors had reported either equal prevalence or a higher prevalence among females than males. Brookes et al.21 had reported the prevalence of hypertension to be higher in men than women among the younger age group, and higher in women than men among the older people (>60 years).
The prevalence of hypertension varies with alcoholic status among males. In the present study, hypertension was significantly higher among those who consumed alcohol (69.6%) than non-consumers (54.2%) and this has also been observed in other studies. On the other hand, Kokiwar et al.22, 23, 24, 25 & Divan et al studies had not observed any significant association between hypertension and alcohol intake. We had also observed highly statistically significant association between hypertension and physical activity level with regard to type of occupation and similar findings had been reported by authors of others studies. Hypertension was found to be significantly associated with abdominal obesity among females only and this finding is consistent with Madhumitha et al.,26 study. A significant association observed between hypertension and family history of hypertension in this study is also supported by other studies done in India. But Yadav et al.,27 study reported no significant differences in prevalence with respect to family history of hypertension. No significant association was observed between hypertension and educational qualification, marital status, SES, religion, type of family, dietary habits, body mass index, history of smoking and abdominal obesity among males. The limitations of the study were small urban area, and small sample size.28
Conclusion
In this study, the results had showed that the prevalence of hypertension had significantly increased with time and is very high (52.1%) in the urban adult population of Puducherry in South India. Advanced age, male gender, sedentary physical activity, abdominal obesity among females, positive family history of hypertension, alcohol use among males had showed significant association with hypertension. It is essential for our health care system to be proactive in screening people for hypertension and educate them about lifestyle modification and risk reduction.