- Visibility 532 Views
- Downloads 45 Downloads
- Permissions
- DOI 10.18231/j.ijpns.2022.019
-
CrossMark

A pre-experimental study to assess the effectiveness of planned teaching programme on knowledge regarding dental hygiene among school going children of Sultan-ul-Arifeen Senior Secondary School Rainawari Srinagar
- Author Details:
-
 Syed Shahid Siraj *
Syed Shahid Siraj *
-
Syed Arifa
Abstract
Dental hygiene is the practice of keeping the mouth, teeth and gums clean and healthy by regular brushing and flossing and preventive dental care. The main aim of the study was to improve the knowledge and practice regarding dental hygiene using planned teaching programme among students of sultan-ul-Arifeen senior secondary school Rainawari Srinagar.
Objectives: To assess the pre-test knowledge among school going children regarding dental hygiene. 2. To assess the post-test knowledge after implementation of planned teaching programme. 3. To compare the pre-test knowledge with the post-test knowledge regarding dental hygiene.
Materials and Methods: Pre experimental research design was used for the study. The study was conducted on 45 school going children selected by stratified sampling technique. Data was collected regarding sociodemographic background of the samples and knowledge was assessed by administering structured knowledge questionnaire. Collected data was analyzed by descriptive and inferential statistics. Descriptive statistics includes frequency, percentages, mean and standard deviation. Inferential statistics includes chi square and t-test.
Result: The study result showed that the pre-test knowledge of the children of Sultan-ul-Arifeen senior secondary school Rainawari Srinagar was 60% and the post-test knowledge was 94%. In the pre-test study, majority of children (55.44%) had moderate knowledge, (44.44%) had inadequate pre-test knowledge and none of them had adequate knowledge. In the post test study, majority of school going children (95.55%) had adequate knowledge, 4.44% had moderate knowledge and none of them had inadequate knowledge.
Conclusion: From the above findings it was concluded that majority of school going children had adequate post-test knowledge after administration of planned teaching programme regarding dental hygiene.
Implications: Identifying the knowledge and attitude of school going children regarding dental hygiene can help the nurse in anticipating the need to arrange health education sessions for students deficient in knowledge regarding dental hygiene.
Introduction
Every tooth in a man’s head is more valuable than a diamond." Miguel de Cervantes Oral health is an integral component of general health. It is also clear that causative and risk factors in oral diseases are often the same as those implicated in major general diseases. Oral hygiene refers to keeping the mouth, and particularly the teeth, clean and free of dental plaque. Considerable population of children in the developing nations is being affected by tooth decay and most of the time; their proper treatment is given the last priority owing to limited access to oral health services. The high prevalence of dental caries has also caused increase in the absenteeism of school hours and loss of working hours and economy for parents.[1] Dental caries is the major oral health condition in developing countries, affecting 60-90% of the school children and vast majority of adults. In India, the prevalence of dental caries is reported to be 50-60% as evidenced by the study conducted by Swarthy Chanda ran on effectiveness of child to child approach on knowledge regarding practices of oral hygiene among school going children at selected schools of Bangalore.[2] In Jammu and Kashmir, the prevalence of dental caries is reported to be 1.8% up to the age of 5years,1.1% up to the age of 12 years,1.9% up to the age of 15 years,5.7% up to the age of 35 to 44 years,18.4% up to the age of 65 to 75 years as evidenced by the study conducted by Nimranjeet Kaur et al on “Oral Health Profile Of J&K”. Though dental caries prevention in school going children has declined in most of the industrialized countries over the last two decades, but it is still high in developing countries including India. Despite great achievements in overall health of populations globally, problems still remain in many countries all over the world- particularly among under –privileged groups in developed and developing countries.[3]
Health is not complete without oral health and health for all by the year 2025 can only be achieved through the medium of primary health care approach. The concept of dental health under the theme “Health for all by 2025 A.D” is a significant issue among human beings because 95% of all human beings have one or other dental problem at least once in their life time.[4]
Oral disease is a significant burden to all countries of the world. The WHO approach to improvement of oral health globally is formulated by the World Health Assembly 2007 Resolution "Oral health: action plan for promotion and integrated prevention".[5]
Children who have dental caries in their primary dentition are more likely to have dental caries in permanent dentition. Growing children need proper guidance for healthy growth, upkeep and hygiene of their teeth. Permanent teeth erupt during the school age years. Good dental hygiene and regular attention to dental caries are vital parts of health supervise during this period. Correct brushing techniques and the role of fermentable carbohydrates in production of dental caries should be taught or reinforced. The objective of this study is to identify oral hygiene practice patterns among school going children. Oral health promotion through schools is recommended by the World Health Organization (WHO) for improving knowledge, attitude, and behaviour related to oral health and for prevention and control of dental diseases among school children.
Age is an important factor for maintaining oral hygiene, as increasing the age children can realize the importance of care of teeth and they emphasize on oral hygiene maintenance. Parents, teachers, other Personnel’s and media are important factors to motivate the children to maintain oral hygiene. The role of self-perception of health status, especially in early schooling years, may need to be explored further as those with more positive perceptions were seen to have more correct oral hygiene practices. This warrants a multi-pronged, multi-level intervention integrating oral health into the school curriculum beginning early schooling is needed.[6]
School is a place of learning for the children and is in fact micro cosmos of the larger community. Schools are the ideal setting for integrating oral health instruction in their curriculum. Health education to school children in their formative age is the most effective method for protection and promotion of their health. Children in schools and family need to be considered as partners in spreading health messages which are beneficial for them. At the school age, children are receptive to guidance and familiar with the learning environment and culture. Oral diseases are largely preventable; nevertheless dental carries continue to be a major problem amongst school children.[7]
The need of this study is that tooth loss, dental caries or cavities is a global problem not only in children but also in adults. The incidence and prevalence of permanent damage or caries in teeth have been increasing day by day, although tooth decay is preventable. Teeth can last a lifetime if we take care of them right and the best to start as they begin appearing. School going children is the period where permanent tooth begins to erupt & children who had caries in their primary dentition will likely to have caries in their permanent dentition. Growing children need proper education and even proper guidance. The foundation for permanent healthy teeth is laid during early childhood. With the eruption of the first permanent teeth (from about 6 years on), the mouth contains a mixture of both primary and permanent teeth, which puts children at increased risk of caries. Furthermore, any primary teeth with caries form reservoirs of bacteria, which can easily attack the immature enamel of the new permanent teeth.
The researcher chose this study because considerable population of children in the developing nations is being affected by tooth decay and less focus is given on its treatment so the study was conducted to assess and deliver the knowledge regarding dental hygiene, proper technique for brushing, prevention from dental caries and management of dental problems. Maintaining dental hygiene in early stage of life can prevent major dental problems later. School is a place of learning for the children and is an ideal setting for integrating dental health instructions. Moreover the oral diseases are largely preventable nevertheless dental caries continue to be a major problem among school children.
Problem Statement
A Pre-experimental study to assess the effectiveness of planned teaching program on knowledge regarding “dental hygiene” among school going children of sultan-ul-arifeen senior secondary school rainawari Srinagar.
Objectives
To assess the pre-test knowledge among school going children regarding dental hygiene.
To assess the post-test knowledge after implementation of planned teaching programme.
To compare the pre-test knowledge with the post– test knowledge regarding dental hygiene.
Hypothesis
H0: There will be no significant difference between pre test and post test knowledge score regarding dental hygiene among school going children.
H1: There will be significant difference between pre-test and post-test knowledge score regarding dental hygiene among school going children.
Assumptions
The school going children have no knowledge regarding dental hygiene.
The knowledge increases after giving planned teaching program regarding dental hygiene.
Delimitation
The study is delimited to the school going children of Sultan-ul-Arifeen Senior Secondary School Rainawari Srinagar who were available at the time of data collection and gave response to the planned teaching programme.
Research approach
The research approach is the umbrella that covers the basic procedure for conducting research. Research approach is the basic procedure for the research enquiry. The research approach helps the researcher to determine what data to collect and how to analyze it. In view of the nature of problem under study and to accomplish the objectives of the study quantitative approach was found to be appropriate to determine the effectiveness of PTP on knowledge regarding dental hygiene among school going children of sultan ul arifeen senior secondary school kathidarwaza srinagar.
Quantitative approach was adopted in the study to find the effectiveness of structured teaching programme on knowledge regarding dental hygiene among school going children of Sultan-Ul-Arifeen Rainawari Srinagar.
Research design
It is a plan of how, when and where data is to be collected and analysed.
It is the researcher’s overall plan for answering the research questions or testing the research hypotheses.[8]
Pre- experimental one group pre test and post test design is adopted for this study.
|
Group |
Pre test assessment of knowledge |
Structured teaching programme |
Post test assessment of knowledge |
|
45 selected samples of school gping children in a selected school |
O1 |
X |
O2 |
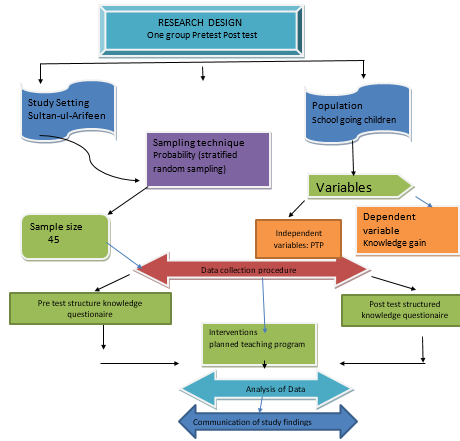
Variables of The Study
Variables
Are the attributes or characteristics that can have more than one value, such as height or weight.[9]
Dependent variables
Variables that change as the independent variable are manipulated by the researcher.[10]
In this study independent variable was Knowledge regarding dental hygiene.
Independent variables
Variables that are purposely manipulated or changed by the researcher. Structured teaching programme was the independent variable in this study.[11]
Setting of the study
location for conducting research,can be natural, partially controlled or highly controlled.[12]
The study was conducted in Sultan-ul-Arfeen Hr sec school Kathidarwaza Srinagar.
Study population
Target population: The entire population in which the researchers are interested and to which they would like to generalise the research findings.[13] The target population of the study was the children who are studying in the Sultan-ul-Arifeen School Rainawari Srinagar.
Accessible population: The aggregate of cases that conform to designated inclusion or exclusion criteria and that are accessible as subjects of the study.[14]The accessible population of the study were all the children who are studying in Sultan-Ul-Arifeen School Srinagar.
Sample: A part or subset of population selected to participate in research study.[15]
Samples were taken from Sultan-ul-Arfeen school. In this study the sample consists of school going children who met the inclusion criteria.
Sample size
Sample size consisted of 45 school going children.
Sampling technique
Stratified random sampling technique was selected for this study.
Stratified sampling is a method of sampling that involves dividing a population into smaller groups-called strata. The groups or strata are organized based on the shared characteristics or attributes of the members in the group.
Criteria for selection of sample
The sample was selected based on following criteria:
Inclusion criteria
The study includes, Children between 12 to 15 who were studying in the school and were present at the time of study.
Exclusion criteria
The study excludes, Children below 12years and above 15 years of age and who were absent at the time of study.
Research tool and technique
Research tool is defined as vehicles that broadly facilitate research and related activities." Research tools" enable researchers to collect, organise, analyse, visualise and publicized research output.[16]
The tool consisted of two parts:
Part 1: Demographic data consisted of following: Age (in years), Gender, Educational status of mother, Family income per month.
Part 2: Structured knowledge questionnaire regarding dental hygiene. The structured questionnaire contains 45 Questions.
|
Part 1 |
Part 2 |
|
Demographic data |
Structured knowledge questionnaire (45questions) |
|
Section A |
Section B (Q.1 to 13- Anatomy and Physiology of teeth) |
|
Age (in Years) |
Section C (Q.14 to 28- dental problems) |
|
Gender |
Section D (Q.29 to 40- Management) |
|
Educational status of mother |
|
|
Family income per month |
|
The different level of knowledge is categorized as follows
|
S. no |
Grade |
Score |
Percentage |
|
1 |
In adequate |
<20 |
<50% |
|
2 |
Moderately Adequate |
20-30 |
51-74% |
|
3 |
Adequate |
>30 |
>75% |
Preparation and development of planned teaching programme
Preparation of PTP
The PTP was prepared based on objectives of the study, literature reviewed and opinion of the experts.
Development of PTP
The steps involved in the development of PTP were.
Review literature.
Preparation of the first draft of PTP regarding dental hygiene.
Experts did content validity and suggestions were considered.
Preparation of final draft.
Editing of PTP.
Selection of content of PTP
The content on dental hygiene was selected through literature search and in consultation with the experts.
The prepared plan was submitted to experts for establishing content validity. Experts suggested simplying the language and rearranging certain areas of plan.
Method of Teaching
Lecture and discussion method was used as appropriate method of teaching dental hygiene to the school going children at Sultan-ul-Arfeen school. The A.V. aids used during teaching the dental hygiene were pictures and videos. The evaluation of PTP was conducted through post test after 5 days of the implementation of the PTP by using structured knowledge questionnaire.
Testing of the tool
Validity of the tool
Validity is defined as the extent to which an instrument accurately reflects the abstract construct (or concept) being examined.[17]
The tool was developed by the investigators and was evaluated by experts from the field of nursing and medicine and it was modified according to their suggestion.
Reliability of the tool
The degree of consistency or accuracy with which an instrument measures the attribute it is designed to measure.[18]
The tool was tested for reliability during pilot study by using split half method. The reliability value of the tool was 0.99 and hence the questionnaire was found to be reliable.
Ethical consideration
The permission had been obtained from the authorities of the BiBi Halema College as well as the authorities of Sultan-ul-Arifeen school Srinagar. The confidentiality of information and annonimity of study subjects was maintained throughout the study.
Pilot study
Study carried out at the end of the planning phase of research in order to explore and test the research elements to make relevant modifications in research tools and methodology.
In order to test the feasibility, relevance and practicability of the study, pilot study was conducted among 45 school going children who are studying in Sultan ul Arifeen school Srinagar. The data was analysed to find out the reliability, it was found 0.99.
Data collection procedure
The formal permission from the principal of Sultan-ul-Arifeen Srinagar was obtained to conduct the study. The investigators introduced themselves to the children of Sultan-ul-Arfeen School and established rapport with them. Pre-experimental one group pretest posttest design was used for the study. A total number of 45 children were selected through stratified random sampling technique. Appropriate orientation was given to the children about the aim of the study, nature of questionnaire and adequate care was taken for confidentiality and annonimity.
The pre test was conducted by using planned questionnaire that consists of part I Demographic data and part II MCQs. A time limit of 40 minutes was taken to each child for pre test. The pre test was conducted in a big hall. After completion of pre test, the investigator gave introduction and followed a planned Teaching Programme for 45 minutes by using PPT. After PPT, their doubts were cleared. The post test was conducted after a period of 6 days using the same questionnaire. The same procedure was followed by all the 45 children.
Plan for data analysis
The data analysis was done according to the objectives of the study. Both descriptive and inferential statistics were used. Statistical analysis of the data was done by the following steps:
Organization of the data in the master sheets.
Frequency and percentage was used to analyze demographic characteristics.
Calculation of mean, standard deviation and mean percentage of scores.
Correlation co-efficient and paired t-test to find out the relationship between pre and post test knowledge.
Summary
The study was pre-experimental in nature and was conducted in Sultan-ul-Arfeen school. The sample for the study were the school going children who were selected by stratified random sampling technique. A structured self administered questionnaire was prepared and the same questionnaire was used to collect the information in both stages of the study. The collected data was analysed by using descriptive and inferential statistics and was presented in the form of tables and graphs.
Descriptive Statistics
Frequency and percentage were used to describe sample characteristics.
Mean, Median, Mode, Range and Standard deviation were used to assess the knowledge of respondents.
Inferential Statistics
Wilcoxon signed Rank test was used to compare pre-test and post-test knowledge.
Organization and presentation of data
The data and the findings were entered in a master data sheet followed by the analysis and interpretation using descriptive and inferential statistics according to the study objectives.
The data and the findings were organized and presented under following sections.
Section1: Description related to distribution of respondents as per their demographic data.
Section2: Description of pre-test knowledge regarding dental hygiene.
Section3: Description of post-test knowledge regarding dental hygiene.
Section4: Comparison between pre-test and post-test knowledge among school going children at Sultan-ul-Arifeen Senior Secondary School Rainawari, Srinagar.
Section I: Description related to distribution of respondents as per their demographic data.
|
Age |
Frequency |
Percentage |
|
13 |
4 |
8.8 |
|
14 |
16 |
35.5 |
|
15 |
12 |
26.6 |
|
16 |
8 |
17.7 |
|
17 |
5 |
11.11 |
[Table 6] Shows that highest percentage 35.5% of the respondent’s were in the age group of 14 years, 26.6% of respondents were 15 years, 17.7% of respondents were 16 years, 11.11 % were 17 years and only 8.8% belong to 13 years of age.
|
Gender |
Frequency |
Percentage |
|
Male |
20 |
44.44 |
|
Female |
25 |
55.55 |
[Table 7] Shows that 55.55% of the respondents were females and 44.44% of the respondent were males.
|
Mothers education qualification |
Frequency |
Percentage |
|
Illiterate |
6 |
13.3 |
|
Matriculate |
14 |
31.11 |
|
Under graduate |
12 |
26.66 |
|
Graduate/pg |
13 |
28.8 |
|
Farhers occuption |
Frequency |
Percentage |
|
Farmer |
2 |
4.4 |
|
Govt employee |
20 |
44.44 |
|
Employee in private sector |
9 |
20 |
|
Business man |
14 |
31.11 |
|
Previous source of information |
Frequency |
Percentage |
|
Health personal |
15 |
33.33 |
|
Mass media |
5 |
11.1 |
|
Senior |
5 |
11.1 |
|
Teacher |
20 |
44.4 |
[Table 10] Bar diagram showing distribution of respondents as per previous source of information.
[Table 10] Reveals that 44.4% of respondents had gained knowledge through teachers, 33.3% had gained knowledge through health personnel, 11.1% of respondents had gained knowledge via mass media and 11.1% had gained knowledge through seniors.
Section II: Description of pre-test knowledge regarding dental hygiene among school going children at Sultan-ul-Arifeen Senior Secondary School Rainawari, Srinagar.
Frequency and percentage distribution of respondents as per their knowledge during pre-test regarding dental hygiene.
|
Grade |
Number |
Percentage |
|
In adequate |
25 |
55.55 |
|
Moderately adequate |
20 |
44.44 |
|
Adequate |
0 |
0 |
[Table 11] Shows that 55.55% of the respondents had inadequate knowledge regarding dental hygiene, 44.44% of the respondents were had moderately adequate knowledge and none of the respondents had adequate knowledge.
Section III: Description of post-test knowledge regarding dental hygiene among school going children at Sultan-ul-Arifeen Senior Secondary School Rainawari, Srinagar.
Frequency and percentage distribution of the respondents as per their knowledge during post-test regarding dental hygiene.
|
Grade |
Number |
Percentage |
|
Inadequate |
0 |
0 |
|
Moderately adequate |
2 |
4.445 |
|
Adequate |
43 |
95.555 |
[Table 12] Shows that maximum (95.55%) of the respondents having adequate level of knowledge regarding dental hygiene, 4.445% of the respondents were having moderately adequate knowledge and one of the respondents were having inadequate knowledge.
|
S. no |
Grade |
Score |
Percentage |
|
1 |
In adequate |
<20 |
<50% |
|
2 |
Moderately Adequate |
20-30 |
51-74% |
|
3 |
Adequate |
>30 |
>75% |
[Table 9] Categorizes the score obtained into three grades with score less than 50% labeled as inadequate and a score above 75% as adequate. Anything between these is labeled as moderately adequate.
Section IV: Comparison between pre-test & post-test knowledge among school going children at Sultan-ul-Arifeen Senior Secondary School Rainawari, Srinagar.
|
Grade |
Pre-test |
Post-test |
||
|
Number |
%Age |
Number |
%Age |
|
|
Inadequate |
25 |
55.55 |
0 |
0 |
|
Moderately adequate |
20 |
44.44 |
2 |
4.445 |
|
Adequate |
0 |
0 |
43 |
95.555 |
It shows that in the pre-test 25(55.55%) students had inadequate knowledge, 20(44.44%) had moderately adequate knowledge and none had adequate knowledge regarding dental hygiene among School going children at Sultan-ul-Arifeen Senior Secondary SchoolRainawari, Srinagar. after the administration of Planned teaching programme on knowledge regarding dental hygiene among respondents, almost all the students i.e. 43 (95.555%) showed adequate knowledge, 2 (4.445%) showed moderately adequate knowledge and none of the respondents showed inadequate knowledge in post-test analysis. This means that there was a significant improvement in the knowledge regarding the dental hygiene with a p-value of <0.000.
|
Pre-test |
Post-Test |
||
|
Score |
%Age |
Score |
%Age |
|
822 |
45.66 |
1692 |
94 |
It shows that in the pre-test the total score achieved by the study group was 822 out of 1800 which is 45.66% and the score improved to 1692 which is 94% in the post-test analysis. This shows a significant improvement of knowledge by 48.34%. This means that there was a significant improvement in the knowledge after the administration of planned teachingprogramme.
Data intrepration
In order to compare the pre-test and post-test knowledge regarding dental hygiene among school going children at Sultan-ul-Arifeen Senior Secondary School Rainawari, Srinagar, we will check the normality of the data so that appropriate test can be used. If the data is normally distributed, we will use t test otherwise its alternative test i.e., Wilcoxon signed Rank test will be used.
|
Descriptive Statistics |
|||||
|
|
N |
Mean |
Std. deviation |
Minimum |
Maximum |
|
Pre-test |
45 |
18.2667 |
5.15850 |
10 |
29 |
|
Post-test |
45 |
37.600 |
3.15076 |
25 |
40 |
|
|
Kolmogorov-smirnov test |
Shapiro-wilk test |
||||||
|
Statistics |
d.f |
P value |
Interpretation |
Statistics |
d.f |
P value |
Interpretation |
|
|
Pretest |
0.113 |
45 |
0.185 |
Normally distributed |
0.961 |
45 |
0.131 |
Not Normally distributed |
|
Posttest |
0.239 |
45 |
0.000 |
Not Normally distributed |
0.721 |
45 |
0.000 |
Not Normally distributed |
From the above table it is evident that the Post-test data is not normally distributed, so we have to think alternative of paired t test i.e., Wilcoxon Signed Rank test to compare pre-test and post-test knowledge.
|
Z Value |
P value |
Interpretation |
|
-5.844 |
0.000 |
Highly significant |
Result
From the above table it is evident that there was a significant improvement in knowledge regarding subject dental hygiene among school children after the introduction of planned teaching programme with t=-5.844, p<0.000.
Major findings of the study
Findings related to demographic variables;
In the present study, it was found that out of 45 students, 25 were females and 20 were males.
Findings related to pre test
In the pretest study it was found that majority of students (55.55%) had inadequate knowledge regarding dental hygiene.
Findings related to post test
In the post-test study, majority of students (95.5%) had adequate knowledge regarding dental hygiene.
Findings related to effectiveness of structured teaching program:
After the administration of structured teaching program, knowledge regarding dental hygiene had adequately increased among students ,so the structured teaching program proved to be very effective.
Conclusion
The following conclusion was drawn based on the findings of the study:
As per the pretest knowledge score, it was found that the mean value was 18.2667, mean percentage was 45.66 and range of score was between 10 -29. As per the posttest knowledge score, it was found that mean value was 37.60, mean percentage was 95.55, range of score was between 25-40. The mean difference between the pretest and posttest level of knowledge was 19.34. The calculated z value is -5.844 and p value is 0.000 which was highly significant.
Hence, it can concluded from above the findings that majority of students had adequate post-test level of knowledge after administration of planned teaching programs regarding dental hygiene.
The research hypothesis is accepted. It shows that knowledge of students significantly increased.
Source of Funding
None.
Conflict of Interest
None.
References
- . Dental-hygiene definition. . . [Google Scholar]
- . History of dental hygiene research. J Dent Hyg. 2013;87:1-5. [Google Scholar]
- Saud N, Awal A, Parvin A, Zaman S, Akbar T. Study on Oral Hygiene: Awareness and Practices Among the School Going Children in Rajshahi Division. Res Rev J Dent Sci. 2016;4(2):1-7. [Google Scholar]
- Hadem C, Bhavani B. Effectiveness of Child To Child Approach on Knowledge and PracticeRegarding Importance of Hand Washing Among Primary School Children. RGUHS J Nurs Sci. 2018;8(1):23-8. [Google Scholar]
- . Effectiveness of structured teaching program regarding dental care in increasing the knowledge and practice among children in selected schools t Bangalore,”2012.. . . [Google Scholar]
- Saud N, Awal A, Parvin A, Zaman S, Akbar T. Study on Oral Hygiene: Awareness and Practices Among the School Going Children in Rajshahi Division. Res Rev J Dent Sci. 2016;4(2):41-7. [Google Scholar]
- BT. Effectiveness of Structured Teaching Programme on Knowledge Regarding Oral Hygiene among School Children in St. Bennedict School, Bangalore. Int J Nursing Care. 2019;7(2):8-15. [Google Scholar]
- Suresh K, Sharma. . Nursing Research and Statistics. . [Google Scholar]
- Suresh K. Nursing Research & Statistics. . 2018. [Google Scholar]
- Suresh K. Nursing Research and Statistics. . 2018. [Google Scholar]
- Suresh K. Nursing Research and Statistics. . 2018. [Google Scholar]
- Suresh K. Nursing Research and Statistics. . 2018. [Google Scholar]
- Sharma SK. Nursing Research and Statistics. . 2018. [Google Scholar]
- Ansari J. A text book of medical surgical nursing. . 2018. [Google Scholar]
- WW. a cross-sectoinal study to determine the prevalence and factors associated with dental caries and periodontal diseases in Brazalian children and Adolescents with cerebralpalsy . Int J Environ Res Public Health. 2015;52(4):235-53. [Google Scholar]
- Renatasoares, Wilton W. A cross-sectoinal study to determine the prevalence and factors associated with dental caries and periodontal diseases in Brazalian children and Adolescents with cerebralpalsy. Int J Environ Res Public Health. 2020;276(1):927-35. [Google Scholar]
- Suresh K. A cross-sectional study on prevalence of dental caries and treatment needs in children in coastal areas of West Bengal. J Contemp Clin Dent. 2013;4(4):482-7. [Google Scholar]
- Suresh K. Knowledge and Practice of Preventive Measures for Oral Health Care among Male Intermediate Schoolchildren in Abha, Saudi Arabia. Int J Environ Res Public Health. 2020;17(3). [Google Scholar]
- Abstract
- Introduction
- Problem Statement
- Objectives
- Variables of The Study
- Variables
- Dependent variables
- Independent variables
- Setting of the study
- Study population
- Sample size
- Sampling technique
- Criteria for selection of sample
- Research tool and technique
- Preparation and development of planned teaching programme
- Development of PTP
- Selection of content of PTP
- Method of Teaching
- Summary
- Descriptive Statistics
- Inferential Statistics
- Result
- Conclusion
- Source of Funding
- Conflict of Interest
- References