- Visibility 588 Views
- Downloads 21 Downloads
- DOI 10.18231/j.ijpns.2022.018
-
CrossMark

Nifty cup versus katori-spoon feeding in preterm infants – Study protocol of a randomized controlled trial
- Author Details:
-
 Neetu Gujjar
Neetu Gujjar
-
Geetanjli Kalyan *
-
Jogender Kumar
-
Praveen Kumar
Introduction
Prematurity is a global problem and a major contributor to neonatal mortality. Maintaining good nutrition is a big challenge among preterm neonates related to their anatomical and physiological immaturity.[1] World Health Organization (WHO) recommends using the cup, Katori- spoon or paladai for feeding the low birth weight who has not developed mature Oro-motor reflex infant cue to determine the frequency and duration of feeding.[2] WHO also discourages using pacifiers, teats, and bottles to decrease the chances of nipple confusion and delay in initiating breastfeeding. In the past, many artificial techniques were used to feed infants, like pap bowls, feeding horns, cups with lips, spouts, and bottles.[3] But most of these feeding techniques are not being used nowadays. Bottles, Katori-spoon, paladai, and cups have dominated all other feeding techniques. In different cultures, different methods for oral feedings are used.
Numerous research has been conducted comparing these methods to determine the most effective method of feeding preterm neonates. Despite showing the benefits of an alternative feeding method, all these previous studies also highlighted some issues arising from these methods, like duration of feeding with a spoon, refilling for paladai, and chances of pouring the milk into the infant's mouth.[4], [5], [6], [7], [8] Cup feeding has been considered a better method to feed preterm neonates regarding safety and physiological stability, but the problems like longer feeding duration, spillage, compliance, and acceptability are reported with its use.[9] To overcome these issues, a new cup NIFTY cup has been developed by Laerdal Global Health.[10] There is not enough evidence to support its efficacy. So, there is a need to conduct more studies on its use.
Need of The Study
The practice of feeding the preterm neonate varies in different settings. In our setup, Katori-spoon feeding is routinely deployed for feeding preterm infants. The use of the Nifty cup has just begun. Recent studies showed it as a promising tool compared to medicine cups and paladai. We searched Medline (via PubMed), CINHAL, Scopus, and Cochrane library for studies comparing the efficacy and safety of the Nifty cup and found only 2 studies on Nifty cup use in infant feeding. One compared the Nifty cup with paladai, and another compared it with a traditional medicine cup.[9], [10] However, until now, no study has compared the Nifty cup and traditional Katori-spoon feeding.
Materials and Methods
Research question
Our research question is whether the Nifty cup, as compared to traditional Katori-spoon feeding, achieves full oral feeds (150 mL/kg/day) earlier in preterm infants (< 34 weeks gestational age at birth) on gavage feeds?
Aim of the study
The present study aiims to compare NIFTY cup vs. Katori-spoon feeding in terms of time taken to reach full oral feeds, duration of feeding transition, spillage,adverse events and anthropometry among preterm neonates admitted in the Neonatal unit, Nehru Hospital, PGIMER, Chandigarh 2020-2022.
Variables
Primary variable
To compare the time taken to reach full feed and the duration of feeding transition (150ml/g/day)
Secondary variables
The secondary outcomes will be (i) time to attain full breastfeeds, (ii) time spent during the feeding sessions, (iii) spillage of feeds, (iv) adverse events (including mortality), (v) anthropometry (weight, length, occipitofrontal circumference) at discharge, (vi) duration of hospitalization. We will also take the opinion of mothers/caregivers and nurses on Nifty cup use
Operational definitions
(i)Transition to complete oral feed- It will be estimated from the 1st day after initiating feeds via the allocated method till the day neonate can take feed 150ml / kg/ day. The gavage tube will be removed when the baby reaches 150 ml/kg Katori spoon feed and tolerates it for consecutive 2 days.*Time to reach full breastfeeding will be estimated in a similar way
(ii) Duration of feeding (minutes) – It is started when the cup/spoon first touches the neonate's lip until the feed completion, i.e., when it last touches the neonate's lip. Mothers will be taught to record the feeding duration of 2-3 feeding session per day, and Primary investigators will also record 2-3 feeding sessions per day. It will be recorded in the treatment chart of neonates.
(iii) Adverse events- These are any unintentional harmful events that can happen during feeding a preterm neonate and includes: aspiration, choking, gagging, bradycardia, regurgitation, apnoea, injury, vomiting and will be assessed from records. Apnoea is the pause in breath for > 20 sec during feeding or of lesser duration if associated with bradycardia/cyanosis. Bradycardia is a heart rate < 100 /min sustained for > 20 sec during feeding.
(iv) Spillage(grams) – A non-permeable cotton cloth (bib) placed around the neck of the neonate before feeding. Spillage will be the difference in the pre and post-feeding weight of the cotton cloth/bib. From the total no. of feeding/day, 2-3 of feedings will be assessed by 1st investigator and will be recorded in the daily feeding chart of the neonate.
The study will be conducted at a step-down unit of a level III neonatal unit of a tertiary care center in Northern India. Ethical consideration has been taken from the institute ethics committee. Preterm neonates born before 34 weeks of gestational age and on orogastric/ nasogastric tube feeding for at least three subsequent days will be eligible for enrolment. They will be included once they are deemed fit for oral feeds and parents are willing to participate in the study. Infants with congenital gastrointestinal and craniofacial malformations like cleft lip, cleft palate, omphalocele, gastroschisis, Tracheoesophageal fistula, esophageal atresia, structural brain malformation, hypoxic-ischemic encephalopathy (grade 3 or 4 IVH), neonatal seizures, necrotizing enterocolitis stage 2 or beyond, severe gastro-esophageal reflux requiring anti-reflux medications, surgical GI malformation, etc. will be excluded.
Randomization
It will be an open-label, parallel-group randomized controlled trial. The trial protocol is registered at the clinical trial registry of India (CTRI/2021/06/034252). We will divide the eligible participants into two stratas as per gestational age (Upto 30 weeks and 31- 330/6 weeks). We will use the block randomization strategy. The person not directly involved in the study will generate the randomization sequence using a web-based platform and construct randomly varying, permuted, even-numbered blocks for each stratum. The block sizes will be concealed until the end of data collection. The concealment will be ensured by using serially numbered opaque sealed envelopes, which will bear a slip of paper with the allocation group.
Sample size
In a previous study with a similar study population, the median (IQR) time to shift the baby from tube to full oral feed (i.e., transition period) was 11 (9-16) days. For a superiority trial, we will need 94 participants to find a significant difference of three days in transition duration with a power of 80% and an α error of 5 %. We will enroll 106 participants considering a 5% chance of non-compliance/crossover in the intervention group.[11] The conceptual framework of this study is built upon the 21 nursing problems theory given by Faye Glenn Abdellah
Intervention and control groups
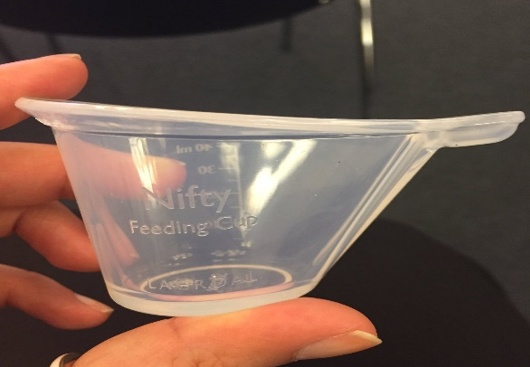
Neonates after enrollment will be randomly assigned to the intervention group (Nifty cup) and the control group (Katori-spoon). The institute will provide the Nifty cup and katori-spoon. The Nifty cup is a 40 ml silicone-made reusable feeding cup for neonates. It has measurement marking and a groove from which the neonate can lap the milk ([Figure 1]). Katori-spoon are reusable steel utensils of variable sizes commonly used in India to feed neonates. The amount of breastmilk is measured with a 10ml syringe.
Nurses will teach the mothers regarding feeding methods and will demonstrate feeding methods until the mothers are confident.
Tools and protocols
The tools used will be (i) Screening sheet of the neonate (ii) Socio-demographic profile of the mother/caregiver (iii) Socio-demographic cum clinical profile of the neonate (iv) Neonate Assessment and follow-up sheet ([Table 1]) (v) feeding chart of neonate (vi) recording sheet for the duration of feeding and spillage (vii) Questionnaire to assess the opinion of mothers (viii) Opinionnaire for feedback of Nurses ([Table 2]). The protocols for Nifty cup feeding will be developed and will be used to train the mothers/ caregivers by nurses.
In addition, the protocol for hand expression of breast milk published in the facility-based newborn care module will be used.[12] The content validity of the tools and protocols is established by giving the tools to seven experts for validity, and all the items were found relevant. Based on their opinions, modifications were made. The reliability of the tool was checked by using Cronbach's alpha and was found to be 0.764
|
Sr. No. |
Neonatal Data |
|
|
1. |
Baby of (Mother’s name) |
|
|
2. |
CR. No. |
|
|
3. |
Sex |
|
|
4. |
Date of Birth |
|
|
5. |
Time of Birth |
|
|
6. |
Gestational age at the time of delivery |
|
|
7. |
Birth weight |
|
|
8. |
Appropriateness for gestational age (Fenton preterm growth chart) |
|
|
9. |
APGAR score |
at 1 minute at 5 minutes |
|
10. |
Postnatal age at enrolment in the study |
|
|
11. |
Post-natal age at the time of intervention |
|
|
12. |
NEC |
|
|
13. |
CRIB score |
|
|
14. |
Clinical diagnosis |
|
|
Sr.no. |
Variables |
N(%) |
|
1. |
Date of enrolment in the study |
|
|
2. |
Mode of feeding before the time of enrolment |
|
|
3. |
Method of feeding as per enrollment |
|
|
4. |
Date of reaching the full oral feed (150mL/kg/day) |
|
|
5. |
Date of initiating breastfeed |
|
|
6. |
Date of reaching full breastfeed |
|
|
7. |
Weight at the time of enrollment in the study (kg) |
|
|
8. |
Weight at the time of discharge (kg) |
|
|
10. |
Length at the time of enrollment (m) |
|
|
11. |
Length at the time of discharge (m) |
|
|
13. |
OFC at the time of enrollment (m) |
|
|
14. |
OFC at the time of discharge (m) |
|
|
15. |
Method of feeding at the time of discharge |
|
|
16. |
Date of discharge |
|
|
17. |
Day of life at the time of discharge |
|
|
|
Questions |
Strongly Disagree |
Disagree |
Neutral |
Agree |
Strongly Agree |
|
Nurses (n=). Compared to Katori-spoon |
||||||
|
1 |
It is easy to train caregivers in administering feeds by Nifty cup. |
|
|
|
|
|
|
2 |
It is easy to feed preterm neonates with Nifty cup. |
|
|
|
|
|
|
3 |
The milk flow control of the baby is better with Nifty cup. |
|
|
|
|
|
|
4 |
It is easier to clean Nifty cup. |
|
|
|
|
|
|
5 |
I will prefer advising use of Nifty cup in future. |
|
|
|
|
|
|
|
Mothers (n=) |
|||||
|
1 |
It is easy to express the milk directly into the cup. |
|
|
|
|
|
|
2 |
It is easy with cup to measure the desired amount of milk to be given to the baby. |
|
|
|
|
|
|
3 |
It is easy is to feed your baby with this cup? |
|
|
|
|
|
|
5 |
It is easy to clean the cup after feeding. |
|
|
|
|
|
|
6 |
I am likely to advise using this cup to my fellow caregivers whose babies need spoon/cup feeding. |
|
|
|
|
|

Pilot study
To assess the feasibility, we did a pilot study among ten neonates (5 in each group). The pilot study indicated that it would be feasible to do the full trial in our setup. This also helped develop standard operating procedures for the initiation and hiking of feeds.
Statistical Analysis
The primary investigator will collect the data using the study flow (Figure 1) and enter it into an excel sheet. We will describe the categorical variables as percentages, normally distributed numerical variables as means (SDs), and those with skewed distributions as medians (1st,3rd quartiles). Skewness will be determined by using the Shapiro-Wilk test and Q-Q plots. We will compare the categorical outcome variables using the χ2 test or Fisher's exact test and numerical variables using the student's t-test or Mann–Whitney U test. Statistical significance will be set at p < 0·05 with two-tailed testing. We will do a linear regression analysis to determine if the intervention is an independent predictor of time to full oral feeds after adjusting for pre-specified variables like gestational age, birth weight, and postmenstrual age (PMA) at enrolment. We will do intention to treat analysis. All data will be analyzed using Statistical Package for the Social Sciences (SPSS) version 23.0 statistical software for Windows.
Discussion
Preterm infants are started on alternative feeding methods until they can initiate breastfeeding. These alternative methods include the usage of Katori-spoon, paladai, and cup feeding. Literature has proven that all these techniques are better than bottle feed. However, there are shortcomings in every method. Problems like refilling with paladai, duration of feeding with cup, and force feed with Katori-spoon are identified.[4], [5], [6], [7], [8] WHO discourages the use of bottle as it can lead to nipple confusion. However, there are variable reports on using paladai, Katori-spoon, and cup feeding methods.
In the present study setting, only spoon-feeding has been used for almost from last 10 years. The paladai was introduced in a research study with n=51. Though the study concluded paladai to be better than the spoon, no attempts were made to bring it to nursing practice, and usage of Katori-Spoon was continued.[6]
The nifty cup is a relatively new cup, and its use has just begun. So, the study will compare Nifty cup and Katori-spoon with the outcome variables above. The study will help generate valuable evidence to feed preterm neonates and benefit preterm neonates, mothers, and health care professionals.
Strengths and Limitations of The Study
The study will be conducted at a tertiary care center with a large number of eligible infants, trained staff, and a robust research methodology. It will be an RCT of adequate sample size for the primary outcome; hence will be able to answer the research question with sufficient power. Due to the nature of the intervention blinding will not be possible for the participants and assessors. Therefore, there is a possibility of performance bias. As our outcomes are mostly objective, the bias might not be significant.
Delimitation of The Study
The study is delimited to stable preterm neonates admitted to the Neonatal unit, Nehru Hospital, PGIMER, Chandigarh.
Implications of the study in nursing
Protocol for feeding the preterm neonate with the NIFTY cup will be prepared, providing a future reference for the mothers, staff, and students caring for preterm neonates. This study will provide empirical evidence about which technique is better for feeding preterm neonates.
Conclusion
The trial will help determine whether Nifty cup feeding is superior to traditional Katori-spoon feeding for preterm gavage-fed infants who are otherwise fit for oral feeding.
Source of Funding
None.
Conflict of Interest
There is no conflict of interest, personal or financial interest that can influence the present study.
References
- J Villar, F Giuliani, ZA Bhutta, E Bertino, EO Ohuma, LC Ismail. International Fetal and Newborn Growth Consortium for the 21(st) Century (INTERGROWTH-21(st)). Postnatal growth standards for preterm infants: the Preterm Postnatal Follow-up Study of the INTERGROWTH-21(st) Project. Lancet Glob Health. Lancet Glob Health 2015. [Google Scholar]
- World Health Organization. Cup-feeding for low-birth-weight infants unable to fully breastfeed. 2020. [Google Scholar]
- S Lang, CJ Lawrence, RL Orme. Cup feeding: an alternative method of infant feeding. Arch Dis Child 1994. [Google Scholar]
- S Deb, A Sharma, C Author, P Gogoi, P Paharia, A Sharma. Cup feeding: an alternative method of infant feeding. Arch Dis Child 2020. [Google Scholar]
- M Marofi, F Abedini, M Mohammadizadeh, S Talakoub. Effect of palady and cup feeding on premature neonates' weight gain and reaching full oral feeding time interval. Iran J Nurs Midwifery Res 2016. [Google Scholar]
- M Kaur, R Kaur, P Kumar. A Study to compare feeding by 'Paladai' and 'Spoon' in terms of efficacy and adverse events in premature neonates (28-32 weeks). Unpublished thesis (hardcopy)Chandigarh: PGIMER;2011. . [Google Scholar]
- KA Marinelli, GS Burke, VL Dodd. A comparison of the safety of cupfeedings and bottlefeedings in premature infants whose mothers intend to breastfeed. J Perinatol 2001. [Google Scholar]
- P Chikoli, N Kumar, R Shenoi, A Comparison. A. Comparison of feeding methods in neonates - a retrospective cohort study from india.. Indian J Child Health 2017. [Google Scholar]
- CM Mckinney, RP Glass, P Coffey, T Rue, MG Vaughn, M Cunningham. Feeding Neonates by Cup: A Systematic Review of the Literature.. Matern Child Health J 2016. [Google Scholar]
- . Nifty Feeding Cup | Laerdal Global Health. 2017. [Google Scholar]
- S Unal, N Demirel, AY Bas, İ Arifoğlu, S Erol. Impact of Feeding Interval on Time to Achieve Full Oral Feeding in Preterm Infants: A Randomized Trial. Nutr Clin Pract 2019. [Google Scholar]
- K Edmond, R Bahl. Optimal feeding of the low-birth-weight infant. Technical review.. World Health Organization 2007. [Google Scholar]
- Introduction
- Need of The Study
- Materials and Methods
- Research question
- Aim of the study
- Variables
- Operational definitions
- Randomization
- Sample size
- Intervention and control groups
- Tools and protocols
- Pilot study
- Statistical Analysis
- Discussion
- Strengths and Limitations of The Study
- Delimitation of The Study
- Conclusion
- Source of Funding
- Conflict of Interest